MedTech Strategist. May 2023 Digital Issue, Celéri Health Creates Foundation for Precision Pain Management
PainIntel ROI Calculator PainIntel ROI Calculator
 According to The National Institute of Mental Health, “People with other chronic medical conditions have a higher risk of depression.”1 To that end, there is a high probability that any person with a chronic pain condition has a concomitant psychological disorder, most notably depression and/or anxiety. The relationship between chronic pain and depression/anxiety is well established. The causal link between pain and these disorders can point in either direction and over time may form a positive feedback loop between these two elements.
According to The National Institute of Mental Health, “People with other chronic medical conditions have a higher risk of depression.”1 To that end, there is a high probability that any person with a chronic pain condition has a concomitant psychological disorder, most notably depression and/or anxiety. The relationship between chronic pain and depression/anxiety is well established. The causal link between pain and these disorders can point in either direction and over time may form a positive feedback loop between these two elements.
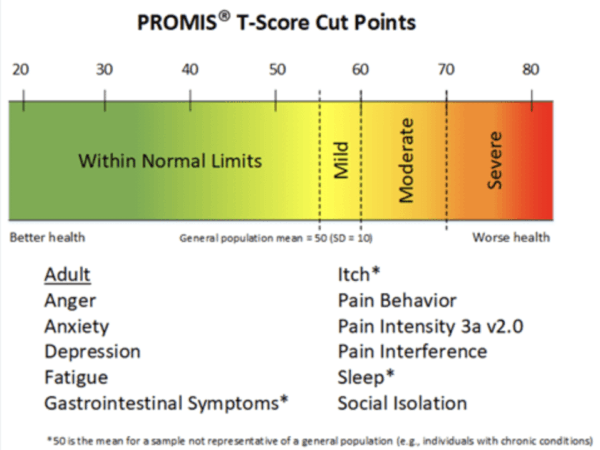
Screening tools are available that will aid in the detection of potential depression/anxiety, and when indicated, a referral may be most appropriate for more extensive evaluation and treatment. In addition, lesser psychological factors such as catastrophizing and fear avoidance behavior may interfere with a patient’s recovery and should be recognized by the clinician. Recognizing indicators of patient psychosocial health behavioral factors can affect a patient’s recovery and/or compliance with treatment and may decrease the risk of developing chronic illness/pain. Tools such as the PROMIS-29, Pain Catastrophizing Scale, and PHQ-9 depression scales are examples.
PainIntel ROI Calculator PainIntel ROI Calculator
May 2023 – MedTech Strategist – Digital Issue Pain is individual, yet the field lacks biomarkers by which clinicians can tailor therapies to their patients. To enable more
The Role of Screening Tools According to The National Institute of Mental Health, “People with other chronic medical conditions have a higher risk of depression.”1
