
Top Pain Assessments and Their Value in Medical Decision Making
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
 Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then every 60 days or Oswestry for all presenting new low back pain or Opioid Risk Tool as a screen for all new patients pending a pharmacology intervention plan.
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then every 60 days or Oswestry for all presenting new low back pain or Opioid Risk Tool as a screen for all new patients pending a pharmacology intervention plan.
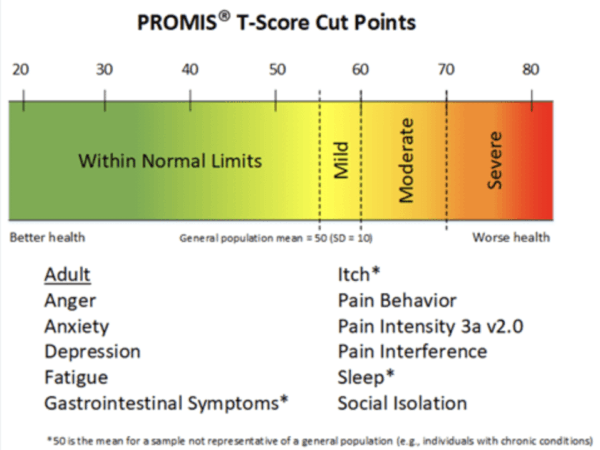
1. PROMIS-29 (Patient-Reported Outcomes Measurement Information System)
Purpose: Evaluates multiple health domains including physical function, pain interference, fatigue, sleep disturbance, anxiety, depression, and social participation.
Clinical Use: Provides a comprehensive profile of a patient’s health status, aiding in identifying areas needing intervention and tracking treatment outcomes.
2. Oswestry Disability Index (ODI)
Purpose: Assesses the degree of disability and functional impairment due to low back pain.
Clinical Use: Helps determine the impact of back pain on daily activities, guiding treatment plans and evaluating patient progress over time.
3. Opioid Risk Tool (ORT)
Purpose: Screens for the risk of opioid misuse in patients being considered for opioid therapy.
Clinical Use: Identifies patients at higher risk for opioid abuse, informing prescribing decisions and the need for monitoring strategies.
4. Numeric Rating Scale (NRS)
Purpose: Measures pain intensity on a scale from 0 (no pain) to 10 (worst possible pain).
Clinical Use: Provides a quick assessment of pain severity, useful for evaluating treatment efficacy and adjusting pain management strategies.
5. PROMIS Prescription Pain Medication Misuse
Purpose: Assesses behaviors indicative of prescription pain medication misuse.
Clinical Use: Aids in identifying patients who may be misusing medications, facilitating timely interventions and adjustments to treatment plans.
6. PHQ-9 (Patient Health Questionnaire-9)
Purpose: Screens for depression and measures its severity based on nine criteria.
Clinical Use: Assists in diagnosing depression, monitoring treatment response, and making informed decisions regarding mental health interventions.
7. GAD-7 (Generalized Anxiety Disorder-7)
Purpose: Screens for generalized anxiety disorder and assesses its severity.
Clinical Use: Facilitates the identification of anxiety disorders, guiding treatment choices and monitoring patient progress.
These tools collectively support pain clinicians in making informed decisions by providing standardized assessments of pain, functional impairment, and mental health status. They enable personalized treatment planning, risk assessment, and monitoring of therapeutic outcomes.
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
 According to The National Institute of Mental Health, “People with other chronic medical conditions have a higher risk of depression.”1 To that end, there is a high probability that any person with a chronic pain condition has a concomitant psychological disorder, most notably depression and/or anxiety. The relationship between chronic pain and depression/anxiety is well established. The causal link between pain and these disorders can point in either direction and over time may form a positive feedback loop between these two elements.
According to The National Institute of Mental Health, “People with other chronic medical conditions have a higher risk of depression.”1 To that end, there is a high probability that any person with a chronic pain condition has a concomitant psychological disorder, most notably depression and/or anxiety. The relationship between chronic pain and depression/anxiety is well established. The causal link between pain and these disorders can point in either direction and over time may form a positive feedback loop between these two elements.
Screening tools are available that will aid in the detection of potential depression/anxiety, and when indicated, a referral may be most appropriate for more extensive evaluation and treatment. In addition, lesser psychological factors such as catastrophizing and fear avoidance behavior may interfere with a patient’s recovery and should be recognized by the clinician. Recognizing indicators of patient psychosocial health behavioral factors can affect a patient’s recovery and/or compliance with treatment and may decrease the risk of developing chronic illness/pain. Tools such as the PROMIS-29, Pain Catastrophizing Scale, and PHQ-9 depression scales are examples.
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
Our most innovative Celéri client providers use RWD from our Real World Outcomes Engine™ in their everyday practice to support care planning and population health. Here are a few ways they do it:
We engage with your patient’s on your behalf over SMS or email or iPads provided in your office – or mobile. Our digital engagement understands that patients need to know they are providing key information directly and securely to their provider. Our messages can look something like this: “Hello Susan, this is Dr. Smith. I am reaching out to understand more about how your pain is impacting your daily life. I want to help. These questions are essential to our custom plan for your pain recovery. Please take a moment to answer them with full candor and then we can discuss your answers when we see each other soon.” Or, your choice of introductory wording. (English and Spanish, available, too)
The majority of our provider clients ask us to gather PROMIS-29 to understand fatigue, pain intensity, pain interference, physical function, sleep disturbance, anxiety, depression, and ability to participate in social roles and responsibilities – as an outcomes baseline and a starting point for patient collaboration in their patient’s pain recovery. Additionally, our Body Map offers visuals for patients to indicate pain areas by primary, secondary and so on – for downstream assessment triggers by body area. Body Map use also helps our provider patients understand our engagement questions are by pain area and not generalized pain – thereby mitigating a possible skewing of PRO results. Of course, ODI or NDI or other validated instruments can be initially gathered also. Our provider clients customize the validated assessments they want and at what cadence. Set it and it works quietly in the background. We deliver the new patient’s PROMIS-29 report (and others) directly to their appointment in your EHR/EMR for your reference before walking in the exam room and as a teaching tool (See Patient Education and Care Planning).
As the patient moves on in their clinical pathway, we gather PRO assessments for our provider’s, based on the intervention in play. At Celéri, it is all about the provider’s choice – based on their preferred PROs by intervention. We have default pathways – or clients can customize their own. For example, many of our client’s SCS patients receive a Zurich Claudication Questionnaire (ZCQ) at -7 days, 7 days out, and 30 days out from trial. Then, at Implant, a cadence of -7 days, 7 days out, 30 days out, 60 days out, 90 days out, 180 days out, 1 year, 2 years, etc. Assessment cadence stops if a known explant occurs, of course. You can change that pathway to add PGIC or PROMIS-29 at any point, if that is your preference. Or, use the IMMPACT recommended outcomes for SCS. For RF or SI Fusion, many of our providers receive ongoing ODIs at -7 days, 7 days out, 30 days out, 60 days out, 90 days out, 180 days out, 1 year, 2 years, etc. Medical management patients can receive our Schedule Substance Abuse Panel (PROMIS Pain Prescription Med Misuse, PROMIS Alcohol Use, PROMIS Appeal of Substance Use, PROMIS Severity of Substance Use) at first appointment and every six months – or Opioid Risk Tool or any of our other 20 validated assessments. Once the intervention pathways are set, they run automatically – yet, can be stopped at any time or augmented to included an ad hoc gather of a GAD-7 or PHQ-4 for example.
Our client providers use the individual PRO assessment result reports (pdfs) that are available in their EHR/EMR from us – for education in the exam room and lean on them for medical decision making support. Please note that both time in education and MDM considerations may have E&M level implications and therefore revenue cycle implications.
After gathering PROs and other custom data elements on patients to support in-clinic visits and pre + post surgical interventions, client providers have access to a Command Center that shows a variety of population-level data elements: a heat-map of pain severity across their market for hot-spotting, patient improvement by appointment type/intervention type (look at what device or technique is performing best in what category), patient response by PRO, patient improvement % by PRO type and much more.
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on

Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on

Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
Celéri’s PainIntel™ offers access to various assessments for clients to use in a pain pathway (algorithm) such as PROMIS®29 for all new patients and then
January 2025 – PRESS RELEASE – January 15, 2025. Conshohocken, PA – Celéri Health has released its AI-applied large language model (LLM), PatientFinder™, for use in
January 2024 – PRESS RELEASE – January 8, 2024. Conshohocken, PA – Celéri Health is pleased to announce its collaboration with Guam Regional Medical City on
